Farmeconomia. Health economics and therapeutic pathways 2026; 27(1): 35-44
https://doi.org/10.7175/fe.v27i1.1607
Original research
Economic evaluation of landiolol vs standard of care for the treatment of patients with sepsis-related tachyarrhythmia in Italy
Filippo D’Amico 1, Matteo Marzaroli 1, Luana Bortone 2, Sonia Tomasso 2, Ilaria Bozzari 3, Laura Vincenzi 3, Alisa M. Higgins 4, Giacomo Monti 1,5
1 Department of Anesthesia and Intensive Care, IRCCS San Raffaele Scientific Institute, Milan, Italy
2 AOP Orphan Pharmaceuticals Italy S.r.l., Pisa, Italy
3 Cencora PharmaLex, Milan, Italy
4 Australian and New Zealand Intensive Care Research Centre, School of Public Health and Preventive Medicine, Monash University, Melbourne, Australia
5 School of Medicine, Vita-Salute San Raffaele University, Milan, Italy
Abstract
INTRODUCTION: Septic shock is frequently complicated by tachyarrhythmias, which are associated with a poorer prognosis and increased intensive care unit stays. Landiolol, an ultra-short acting β-blocker, is effective in controlling heart rate (HR) and controlling cardiac arrhythmias in patients with sepsis. However, economic evaluations of its use remain limited. This study explores the potential economic benefits of landiolol compared to standard of care (SoC) in the Italian acute/emergency care setting.
METHODS: A decision model was developed to evaluate the cost-effectiveness and budget impact of using landiolol versus SoC to manage sepsis-related tachyarrhythmia. In the model, the clinical benefit was expressed in terms of percentage change in patients reaching HR target. The economic model of landiolol was designed based on Landi-SEP trial. Costs were calculated from the hospital perspective and were derived from literature and national tariffs. A deterministic one-way sensitivity analysis was performed to assess the robustness of the cost-effectiveness analysis, and three alternative scenario analyses were performed on the budget impact analysis.
RESULTS: In the cost-effectiveness analysis, the mean total cost per patient was estimated to be €27,632 for those treated with landiolol vs €30,992 with SoC, corresponding to a difference of −€3,360 per patient. Despite pharmacological costs being higher in the landiolol group, patients treated with landiolol had a reduction of costs associated with hospital stay (−€4,251 per patient) compared with SoC. In the budget impact base case analysis, the gradual use of landiolol was associated with a decrease in the overall healthcare expenditure, with cumulative savings of approximately €22.5 million over three years. The projected expenditure for landiolol is offset by the reduction in expenditure on the other healthcare resources included in the analysis, primarily hospital stay.
CONCLUSION: The use of landiolol may reduce hospital costs in the Italian setting. Additional studies are needed to confirm these results in a larger population.
Keywords
Landiolol; Sepsis-related tachyarrhythmia; Cost-effectiveness analysis; Budget impact analysis; Italian healthcare setting
Ilaria Bozzari
Received 18 February 2026
Accepted 14 May 2026
Published 29 May 2026
Introduction
Septic patients are at increased risk of developing cardiac arrhythmias [1,2]. Catecholaminergic vasopressors, necessary to treat physio-pathological hypotension, exacerbate sympathetic nervous system activity, causing increased heart rate (HR) [3]. Tachyarrhythmias during sepsis have been associated with increased mortality and a higher incidence of adverse events [3]. New-onset supraventricular arrythmia was reported in 6% of patients with severe sepsis and in 46% of those with septic shock [4-6], and is associated with an increased length of intensive care unit (ICU) stay among survivors [6]. Conversely, HR control was linked to improved clinical outcomes [7].
Landiolol, an ultra-short acting β-blocker, is indicated for the treatment of supraventricular tachycardia and for the control of ventricular rate in patients with atrial fibrillation or atrial flutter and for non-compensatory sinus tachycardia [8]. Compared with other beta-blockers, landiolol exhibits higher β1-receptor selectivity and a lower hemodynamic impact [9]. Randomized clinical trials have demonstrated that landiolol is effective in reducing HR and preventing new-onset arrhythmias, without increasing vasopressor requirements, compared to standard of care (SoC) including fluid resuscitation, antimicrobial therapy, norepinephrine administration, and corticosteroids [3,8].
Evidence on the economic implications of landiolol use is currently scarce in the published literature. However, understanding its cost implications is important for healthcare decision-making, particularly in the management of critically ill patients with sepsis and tachyarrhythmias. Evaluating whether the higher acquisition cost of landiolol is balanced by reductions in resource utilization—such as shorter hospital stays, fewer complications, or decreased need for additional interventions—is essential to guide clinicians, hospital administrators, and policymakers. In this economic analysis, we aim to evaluate the economic impact of landiolol compared to the SoC.
Methods
Cost effectiveness analysis
Model overview
A decision model was developed using Microsoft Excel to evaluate the cost-effectiveness and budget impact of using landiolol versus SoC to manage sepsis-related tachyarrhythmia (Supplementary Figure 1).
The economic model of landiolol was designed based on Landi-SEP RCT [10]. To date, no clinical trials specifically assessing the efficacy and safety of landiolol in the Italian clinical setting have been published. The Landi-SEP trial, a study conducted at 20 sites in 7 European countries (Czech Republic, Germany, Italy, Austria, Slovenia, Hungary, Estonia), was identified as the most appropriate source to estimate the clinical effects of landiolol compared to SoC [10]. In the model, the clinical benefit was expressed in terms of percentage change in patients reaching HR target. This outcome was selected as it was the primary endpoint, demonstrated statistical significance between comparators, and was validated by clinical experts. Patients with sepsis or septic shock who developed tachyarrhythmia enter the model and received either landiolol or SoC. Within each treatment arm, patients can experience one of two clinical pathways during the modelled time horizon: not achieving the HR target (arrhythmia persists) or no event (successful control). Each of these intermediate health states then leads to one of two final outcomes: death or alive (Supplementary Figure 1).
Resource use was derived from the clinical trial and included the length of stay in ICU and general ward. Hospital length of stay was assumed to correspond to the study time horizon of 28 days. For the landiolol group, length of stay reduction was adjusted according to the hazard ratio of 0.8 reported in the Landi-SEP trial (CI 95% 0.41–1.54) [10]. The model was developed over a time horizon of 28 days in accordance with the available evidence [10,11], which corresponded to the total hospital stay. Due to the short time horizon of the model, discounting of costs was deemed not necessary.
Costs were calculated from the Italian hospital perspective and were derived from literature and national tariffs. Outcomes were expressed as: 1) cost savings; and 2) the incremental cost-effectiveness ratio (ICER), expressed as the cost saved per patient reaching HR target.
The ICER was calculated by dividing the difference in total costs (incremental cost) by the difference in the incremental effect (patients reaching HR target) to provide a ratio of “savings per extra unit of health effect”.
Where applicable, the present economic analysis was conducted and reported in accordance with the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022, which aim to improve the transparency, completeness, and consistency of health economic evaluations [12].
Study outcomes
The primary endpoint was a multi-component endpoint defined by achieving HR response (3 subsequent hourly HR values at 80–94 bpm or < 80 bpm and not clinically relevant), HR maintenance (defined as not recording 3 subsequent hourly HR values > 94 bpm or < 80 bpm after achievement of HR response), and no increase in vasopressor requirements during the first 24 h after treatment [10].
Analysis comparator
Between February 2018 and February 2022, a total of 196 patients were randomly assigned to the landiolol group (n=98) or control group (n=98) [10]. HR response was achieved and maintained in 58.2% and 29.6% of patients respectively in landiolol and control group (Supplementary Table I) [10].
Pharmacological cost and other resource use
Treatment costs were modelled according to the resource use in the Landi-SEP trial. These assumptions were reviewed and validated by clinical experts to ensure their relevance, plausibility, and alignment with current clinical practice. All costs were actualized to 2025 euros using Italian inflation indices [13]. The drug treatments considered included landiolol, norepinephrine, vasopressin, terlipressin, dopamine, and epinephrine. Landiolol was introduced as part of the hypotension treatment to achieve control of tachyarrhythmia. Their utilization was modelled in accordance with the therapeutic regimens reported in the trial. Drug dosages were assumed to correspond to the median doses administered during the study period, as reported in the trial. Supplementary Table II shows the total dose received by the two groups during the whole treatment period. Drug costs were derived from public price lists [15,16]. Due to the short time horizon of the model, there was no discounting of costs.
Resource use data were derived from literature and included hospital stay in general ward and ICU (Supplementary Table III) [10]. Cost per hospital day was derived from administrative databases and literature [17,18].
Sensitivity analysis
A one-way deterministic sensitivity analysis (DSA) was performed to assess how variations of individual input parameter values affected the model outputs, specifically the resulting ICER, and thus to judge the robustness of the study’s findings. Input ranges for sensitivity analysis were obtained by adding or subtracting percentage values (±15%) to or from the baseline estimates.
Budget impact analysis
The objective of the Budget Impact Analysis (BIA) was to compare, in terms of costs and consequences, landiolol vs SoC, from the Italian hospital perspective, for the treatment of adult patients (≥ 18 years old) with sepsis-related tachyarrhythmia.
The BIA aims at estimating, in the short term (3 years), the financial consequences of the adoption and use of a new health technology in a specific territorial area and, therefore, to estimate the impact on the expenditure trend for that condition, following the change in the mix of therapies used.
Two different scenarios were analyzed and compared (Supplementary Figure 2): 1) a scenario without landiolol (current scenario) in which the population is treated with the therapies currently available in Italy for the treatment of patients with sepsis-related tachyarrhythmia; and 2) a hypothetical scenario with landiolol (future scenario) resulting from the introduction and progressive use of landiolol among the options available in Italian clinical practice. Total costs were estimated considering pharmacological costs, hospital stay costs and ICU stay (with or without ventilation) costs. Where applicable, the present economic analysis was conducted and reported in accordance with the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022, which aim to improve the transparency, completeness, and consistency of health economic evaluations [12].
Target population
Literature data estimated a sepsis incidence rate in Italy ranging between 300 and 400 cases per 100,000 inhabitants [19]. Of all care-related infections, 22.5% are classified as septic shock, 20.0% as severe sepsis, and 57% as sepsis only [20]. Considering the incidence of new arrhythmia in the population with severe sepsis and septic shock [4,6], it is estimated that the population eligible for landiolol in Italy is approximately 20,000 patients per year (Figure 1).
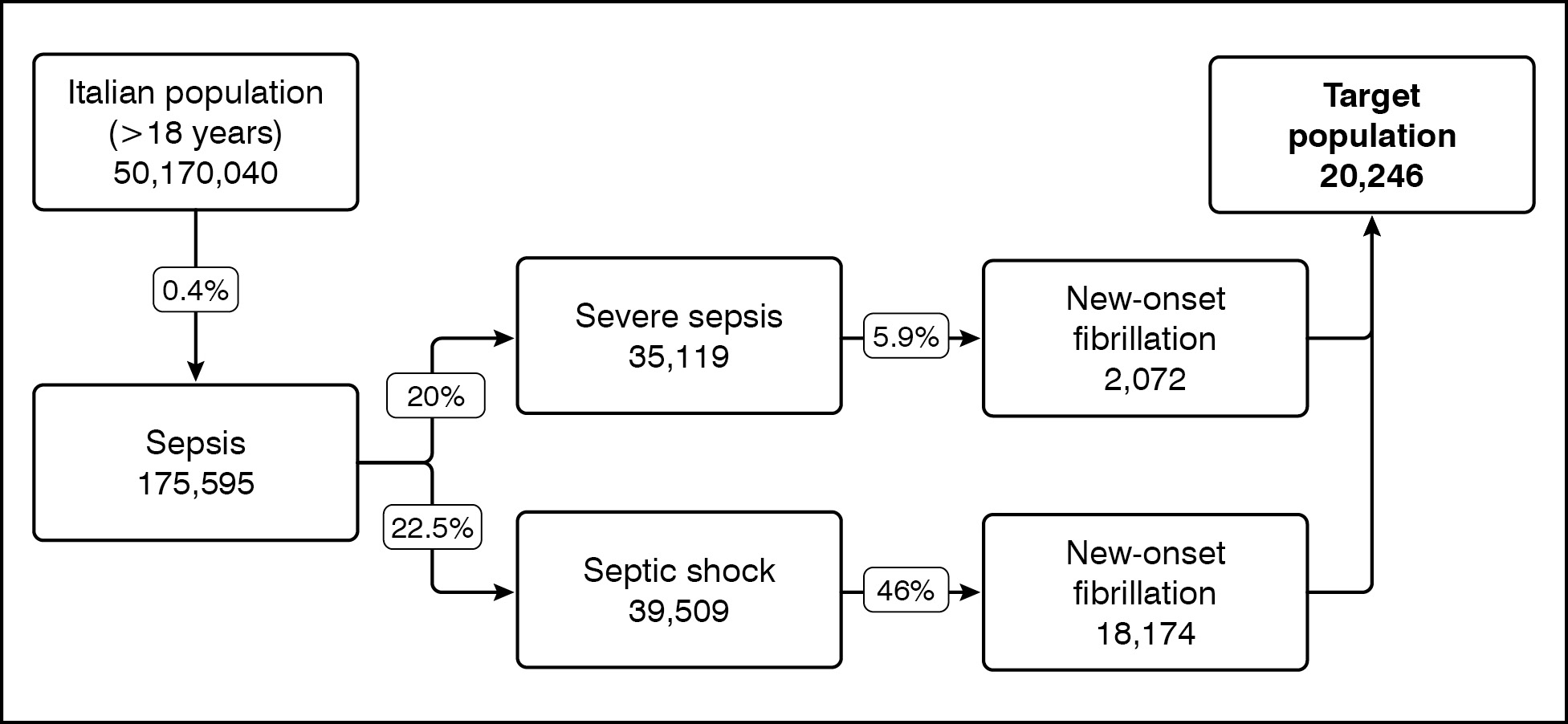
Figure 1. Eligible population for treatment with landiolol
Base case analysis
In the base case analysis, landiolol is not considered among the treatment options in the current scenario; its use is gradually introduced in the future scenario. The distribution of patients by treatments in the current scenario was assessed with market research (Table I) [21]. The estimated treatment mix for the two scenarios of the analysis is shown in Table I. In the future scenario, patients potentially treated with landiolol are estimated to be 1,640 in Year 1, 2,227 in Year 2, and 2,834 in Year 3.
|
Treatment |
Current scenario (%) |
Future scenario (%) |
||
|
Year 1 |
Year 2 |
Year 3 |
||
|
Landiolol |
0.0 |
8.1 |
11.0 |
14.0 |
|
Metoprolol |
8.7 |
7.0 |
6.3 |
5.7 |
|
Esmolol |
15.4 |
14.0 |
13.4 |
12.9 |
|
Amiodarone |
64.1 |
60.0 |
58.6 |
57.1 |
|
Other |
11.8 |
11.0 |
10.7 |
10.4 |
|
Total |
100 |
100 |
100 |
100 |
Table I. Base case analysis: patient distribution by treatment
Clinical and economic inputs
The BIA was performed considering the same assumptions of the cost-effectiveness analysis for clinical efficacy, resource use and costs, except for pharmaceutical cost. The model included landiolol, metoprolol, esmolol, and amiodarone, as well as an “other” category comprising bisoprolol and digoxin (marginal use of additional anti-infective agents). The selection and categorization of treatments were informed by market research data reflecting current clinical practice [21]. Drug costs were derived from public price lists (Supplementary Table IV) [15,16]. Due to the short time horizon of the model, discounting of costs was deemed not necessary. A scenario analysis considering the pharmaceutical costs from cost-effectiveness analysis was performed.
Scenario analyses
Three scenario analyses were performed. Recent market analysis [21] indicates that landiolol is currently used by a small percentage of physicians (< 5%) for the management of sepsis-associated tachyarrhythmia, despite not being reimbursed by the Italian National Healthcare System. Consequently, a scenario analysis was conducted, assuming a 4.6% market share for landiolol in the current scenario. The estimated treatment mix for the scenario analysis is shown in Supplementary Table V.
In alignment with the cost-effectiveness model, an additional analysis has been conducted, considering the treatment distribution from Landi-SEP trial (Table I). This distribution has been considered fixed in the years of analysis.
Finally, a third scenario was developed to assess the economic implications of landiolol when priced considering the latest tender price. This analysis aimed to evaluate the budget impact of landiolol under a hypothetical pricing condition that reflects its proposed acquisition cost.
Results
Cost-effectiveness analysis
Overall, the total cost for patients treated with landiolol was lower than that for patients treated with the SoC (Table II). Despite the higher pharmacological cost, treatment with landiolol was associated with a reduction in hospital stay costs (−€4,251 per patient).
|
Cost components |
Landiolol |
Control |
|
Hospital stay (normal ward) (€) |
5,875 |
10,126 |
|
ICU stay (€) |
20,955 |
20,806 |
|
Drugs (€) |
802 |
60 |
|
Total (€) |
27,632 |
30,992 |
|
Cost difference (€) |
-3,360 |
|
Table II. Results of the cost-effectiveness analysis.
ICU: intensive care unit
Moreover, the analysis showed that each successful case of HR control with landiolol was associated with cost savings of €11,760.
Results of the sensitivity analysis are shown in Figure 2 and were expressed as incremental costs per patients with target HR. The DSA confirmed the robustness of the analysis to variations in the input parameters of the model. In all scenarios analysed, landiolol was cost saving vs SoC. The variations with the highest magnitude of influence were the cost per hospital day (general ward) and the total number of hospital days. This suggests that reductions in overall hospitalization duration associated with achieving target HR have a substantial impact on economic outcomes. Importantly, across all tested parameter variations, incremental costs remained negative, indicating that the intervention was consistently associated with cost savings per patient achieving target HR.
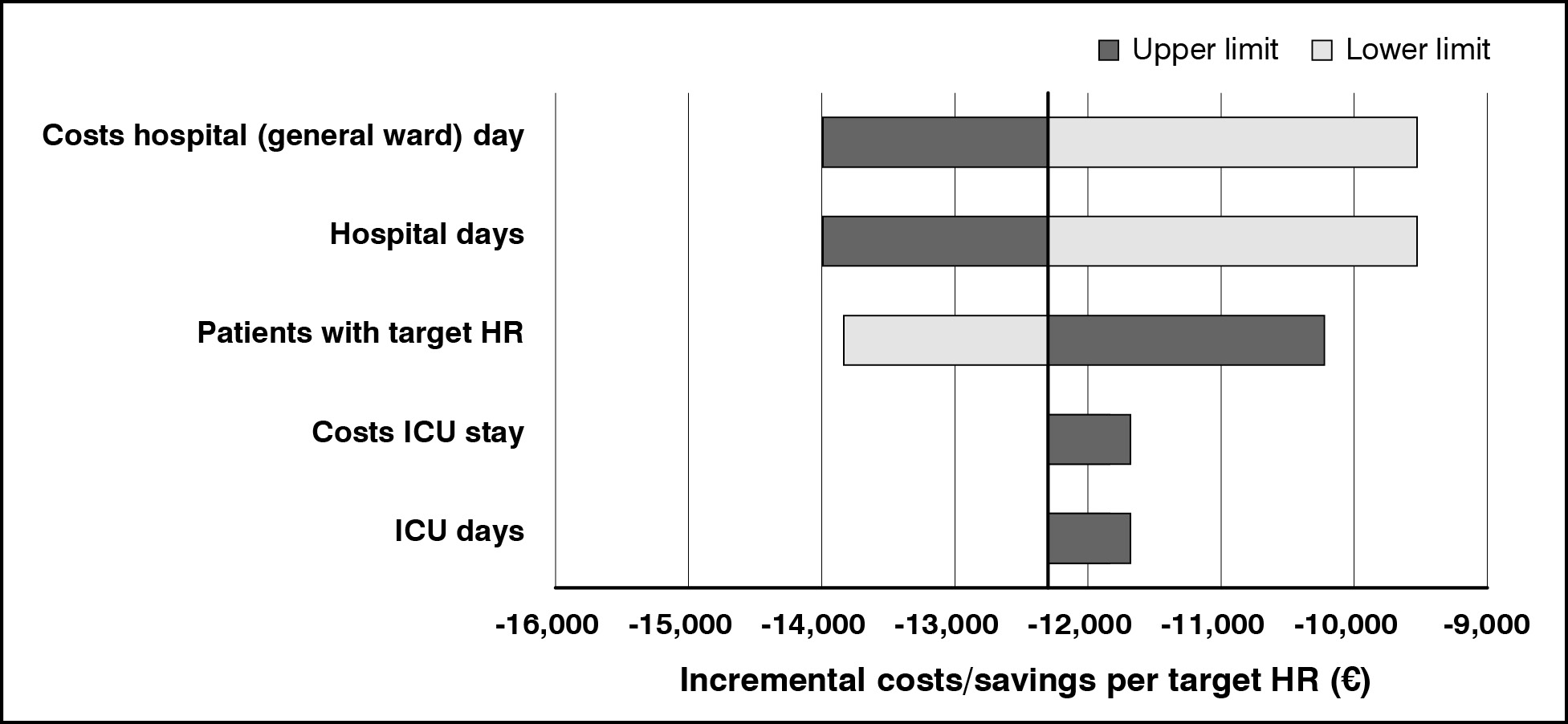
Figure 2. Results of the sensitivity analysis
ICU: intensive care unit
Budget impact analysis
Base case analysis
The results of the base case analysis (Table III) showed that the gradual use of landiolol led to a decrease in the total expenditure. The cumulative savings over the three years was approximately −€22.9 million.
The projected expenditure for landiolol was €1.3 million at Year 1, €1.8 million at Year 2, and €2.3 million at Year 3 and was offset by the reduction in expenditure on the other healthcare resources included in the analysis (hospital stay).
|
Cost Components |
Current scenario |
Future scenario |
||
|---|---|---|---|---|
|
Year 1 |
Year 2 |
Year 3 |
||
|
Hospital stay (normal ward) (€) |
205,014,094 |
198,042,050 |
195,545,886 |
192,963,647 |
|
ICU stay (€) |
421,235,831 |
421,481,300 |
421,569,183 |
421,660,098 |
|
Drugs (€) |
1,460,173 |
2,566,517 |
2,967,634 |
3,385,367 |
|
Total (€) |
627,710,098 |
622,089,866 |
620,082,703 |
618,009,112 |
|
Difference vs current scenario (€) |
- |
−5,620,232 |
−7,627,396 |
−9,700,987 |
Table III. Results of budget impact analysis—base case
ICU: intensive care unit
Scenario analysis
The results of the first scenario analysis (Table IV) confirmed that the increased use of landiolol led to a decrease in expenditure. Although drug acquisition costs increased, cumulative savings over the three years amounted to approximately −€13.3 million.
|
Cost Components |
Current scenario |
Future scenario |
||
|---|---|---|---|---|
|
Year 1 |
Year 2 |
Year 3 |
||
|
Hospital stay (normal ward) (€) |
201,035,994 |
198,042,050 |
195,545,886 |
192,963,647 |
|
ICU stay (€) |
421,375,890 |
421,481,300 |
421,569,183 |
421,660,098 |
|
Drugs (€) |
2,108,601 |
2,585,499 |
2,986,017 |
3,403,131 |
|
Total (€) |
624,520,486 |
622,108,849 |
620,101,086 |
618,026,876 |
|
Difference vs current scenario (€) |
- |
−2,411,637 |
−4,419,400 |
−6,493,610 |
Table IV. Results of budget impact analysis—first scenario analysis
ICU: intensive care unit
The results of the second scenario analysis (Supplementary Table VI) based on treatment distribution from the Landi-SEP trial, further supported these findings. The introduction of landiolol in the treatment paradigm also resulted in cumulative savings of approximately −€22.5 million over three years.
Finally, a third scenario incorporating the tender price of landiolol in the base case was evaluated. This analysis demonstrated additional cost savings, with cumulative reductions in expenditure over the three-year horizon estimated at approximately €24.7 million.
Discussion
In this cost-effectiveness analysis, we found that the use of landiolol was associated with significant cost savings compared with SoC. The cost-effectiveness analysis demonstrated that, despite higher drug acquisition costs, landiolol reduced overall expenditure primarily through shorter hospital stays. Sensitivity analyses confirmed the robustness of these findings, with landiolol remaining cost-saving across all tested scenarios. The findings of the sensitivity analysis are consistent with the published literature, which identifies length of stay, including ICU, as one of the principal cost drivers [22-24]. Furthermore, the budget impact analysis projected substantial cumulative savings over a three-year horizon, ranging from €13.3 to €24.7 million depending on the assumptions applied.
Published health economic evaluations of treatments for sepsis-induced tachycardia are scarce. A recent health economic study explored the cost-effectiveness of using landiolol in the management of sepsis-induced tachycardia in Germany [25].
This study showed that, compared with SoC, landiolol was a dominant strategy over a lifetime horizon, generating cost savings of approximately €2,834 from the German healthcare system perspective and €1,380 from the hospital perspective, while providing a QALY gain of 0.47, equivalent to 5.63 months in perfect health.
To date, no formal economic evaluations have been conducted for esmolol or other agents in the management of sepsis-induced tachycardia. Our analysis is therefore among the first to explore the economic impact of beta-blockade in this clinical setting. There are no recent studies exploring the per-patient cost of sepsis in Italy. A systematic review reported that the median of the mean hospital-wide cost of sepsis per patient worldwide was $32,421 (IQR $20,745–$40,835), which helps to contextualize the magnitude of the savings observed in our analysis [26]. A future reduction in the acquisition cost of landiolol would further enhance its economic value, potentially leading to an even greater impact on healthcare resource utilization.
Our analysis demonstrates the health economic advantages of landiolol in the acute care setting and from the Italian healthcare system perspective. In particular, landiolol reduced costs associated with ICU stay compared with SoC, offsetting the higher medication costs.
Tachycardia is a frequent manifestation in sepsis or septic shock, associated with poor prognosis, hemodynamic instability, and organ dysfunction, thus requiring prompt intervention [19]. Current guidelines, such as the Surviving Sepsis Campaign, emphasize early recognition and stabilization but do not specify which pharmacological agent should be used for rate control [20]. This is mainly due to the lack of strong evidence demonstrating the superiority of one treatment over another in terms of long-term clinical outcomes in patients with sepsis. Nevertheless, the pharmacological profile of landiolol appears promising.
Landiolol leads to a reduction in HR and myocardial oxygen demand, without significantly affecting blood pressure. Landiolol has an onset of action within 0 to 2 minutes after administration and its selectivity ratio (255) is higher than that of other beta-blockers, such as bisoprolol (13.5), atenolol (4.7), metoprolol (2.3), and esmolol (33) [27-29]. Landiolol achieves a more rapid and pronounced reduction in HR than esmolol, without the significant decrease in blood pressure observed with esmolol [9]. Its rapid onset and offset of action make it particularly suitable for acute conditions such as sepsis or septic shock. From a cost–benefit perspective, landiolol appears advantageous, as it combines a favorable hemodynamic profile for clinicians managing septic patients with cost savings for the healthcare system.
This study provides one of the first economic evaluations of HR control in sepsis, addressing a relevant gap in the literature. By drawing on data from randomized controlled trials and incorporating detailed estimates of hospital resource use within the Italian healthcare system, the analysis ensures a high level of internal validity for treatment-effect estimates while offering a realistic assessment of the financial implications of landiolol. The integration of both cost-effectiveness and budget impact analyses, supported by sensitivity testing, ensures that the results are consistent across a range of plausible scenarios. These features increase the credibility of the findings and enhance their value for informing clinical and policy decision-making.
However, the following limitations should be considered when interpreting the results of the present analysis. First, the clinical evidence on landiolol is primarily derived from clinical trials including fewer than 200 patients and is mainly based on HR control, which represents a surrogate endpoint [10]. Future health economic evaluations should include the long-term outcomes, considering that post-discharge mortality following sepsis hospitalization was more common among patients with new-onset AF during sepsis [10]. Although the approach used provides valuable insight into the potential cost savings associated with landiolol use, it does not capture indirect costs or fully account for the complexity of sepsis management. Another limitation is that the clinical efficacy data were derived from randomized controlled trials conducted outside of Italy and then applied to the Italian healthcare context. This may represent a source of bias, as treatment choices in different healthcare systems can be influenced by economic factors and organizational structures that do not necessarily reflect the Italian setting. The absence of real-world data, which are important for confirming applicability in routine clinical practice, also represents an inherent constraint of the study. Another limitation relates to the choice of comparator. In clinical practice, the selection of a specific agent for rate control is not always interchangeable, as clinical factors often determine the preference for one drug over another. The generalizability of our findings should be interpreted with caution, particularly in relation to different healthcare systems. Our analysis was based on data and cost structures specific to the Italian healthcare system, which may limit the applicability of the results to other settings and introduce uncertainty when alternative assumptions are applied. Additionally, the ICER was not expressed in terms of QALYs due to the lack of available utility data; instead, it was calculated as incremental costs or savings per patient achieving the target heart rate. While bootstrapping or probabilistic sensitivity analysis (PSA) was not performed, and therefore confidence intervals around cost estimates and ICERs could not be derived, the DSA of key parameters yielded results consistent with the base-case analysis. This decision not to conduct a PSA was made based on the robustness of results demonstrated through DSA, and the relative simplicity of the analytical model employed.
One-way DSA was performed on all key model parameters. These analyses systematically varied each parameter across its plausible range. The DSA consistently demonstrated that the primary conclusions of the analysis remained stable across all examined parameter ranges. Tornado diagrams revealed that no single parameter, when varied individually, altered the conclusion regarding cost-effectiveness. Given that the DSA comprehensively explored parameter uncertainty space and consistently supported the base-case conclusions, the additional computational burden of a PSA was deemed to provide limited incremental value for decision-making purposes. The analytical framework employed in this study utilized a relatively parsimonious model structure with a limited number of uncertain parameters. Unlike complex Markov models or microsimulation approaches where parameter interactions may generate emergent uncertainty not captured by one-way DSA, our model structure was simple and straightforward. The limited number of uncertain inputs reduced the potential for complex non-linear interactions between parameters that might only be revealed through probabilistic analysis. For models of this level of complexity, the DSA adequately characterized the decision uncertainty without requiring full probabilistic treatment. We acknowledge that the absence of a PSA represents a limitation of this analysis. PSA offers the advantage of jointly varying all uncertain parameters simultaneously, thereby capturing potential correlations and interactions between inputs. This approach also generates valuable outputs such as cost-effectiveness acceptability curves and credible intervals around the incremental cost-effectiveness ratio. These characteristics facilitate interpretation by decision-makers and support informed policy choices. However, in the present analysis, the consistency of the DSA results provides reassurance regarding the robustness of the base-case findings despite the absence of formal probabilistic analysis.
Therefore, the consistency of the clinical evidence on landiolol and the robustness of the sensitivity analyses suggest that similar economic benefits may be observed in comparable healthcare contexts.
While additional evidence would further strengthen current knowledge, existing clinical data indicate that landiolol may represent a valuable therapeutic option in the management of sepsis-induced tachyarrhythmias. Future research should focus on conducting well-designed clinical trials in diverse patient populations and settings, with a particular emphasis on evaluating both clinical and patient-centred outcomes. Additionally, health economic studies should employ comprehensive cost-effectiveness analyses that consider a broader range of factors beyond clinical outcomes alone.
Conclusion
The present economic analyses in the Italian setting show that the use of landiolol can lead to savings in terms of hospital costs. Further studies are needed to confirm the economic impact of landiolol in larger and more heterogeneous patient populations and across different healthcare systems.
Conflict of interest
Cencora PharmaLex received consulting fees from AOP Orphan Pharmaceuticals Italy for conducting the analysis. I.B. and L.V. are Cencora PharmaLex employees. L.B. and S.T. are employees of AOP Orphan Pharmaceuticals Italy, which financially supported the submitted work. G.M. reports personal fees and non-financial support from AOP Orphan Pharmaceuticals Italy outside the submitted work. M.M. reports personal fees from AOP Orphan Pharmaceuticals Italy outside the submitted work. A.M.H. is supported by an NHMRC Investigator Grant (GNT2008447).
Funding
This study was financially supported by AOP Orphan Pharmaceuticals Italy S.r.l.
References
1.Shahreyar M, Fahhoum R, Akinseye O, et al. Severe sepsis and cardiac arrhythmias. Ann Transl Med. 2018;6:6; https://doi.org/10.21037/ATM.2017.12.26
2.Zanotti-Cavazzoni SL, Hollenberg SM. Cardiac dysfunction in severe sepsis and septic shock. Curr Opin Crit Care. 2009;15:392-397; https://doi.org/10.1097/MCC.0B013E3283307A4E
3.Overgaard CB, Džavík V. Inotropes and vasopressors: review of physiology and clinical use in cardiovascular disease. Circulation. 2008;118:1047-1056; https://doi.org/10.1161/CIRCULATIONAHA.107.728840
4.Walkey AJ, Wiener RS, Ghobrial JM, et al. Incident stroke and mortality associated with new-onset atrial fibrillation in patients hospitalized with severe sepsis. JAMA. 2011;306:2248-2255; https://doi.org/10.1001/JAMA.2011.1615
5.Seemann A, Boissier F, Razazi K, et al. New-onset supraventricular arrhythmia during septic shock: prevalence, risk factors and prognosis. Ann Intensive Care. 2015;5:27; https://doi.org/10.1186/S13613-015-0069-5
6.Meierhenrich R, Steinhilber E, Eggermann C, et al. Incidence and prognostic impact of new-onset atrial fibrillation in patients with septic shock: a prospective observational study. Crit Care. 2010;14:R108; https://doi.org/10.1186/CC9057
7.Ning YL, Li WJ, Lu X, et al. Association between heart rate and mortality in patients with septic shock: an analysis revealed by time series data. BMC Infect Dis. 2024;24:1088; https://doi.org/10.1186/S12879-024-10004-Z
8.Agenzia Italiana del Farmaco. Landiobloc 300 mg polvere per soluzione per infusione - Riassunto delle caratteristiche del prodotto. 2022
9.Koukoulitsios G, Tsikritsaki K, Magklaras G, et al. Comparison of landiolol and esmolol on haemodynamic responses during weaning of intensive care unit patients with reduced ejection fraction after vascular surgery. Card Fail Rev. 2025;11:1-6; https://doi.org/10.15420/CFR.2024.18
10.Rehberg S, Frank S, Černý V, et al. Landiolol for heart rate control in patients with septic shock and persistent tachycardia. A multicenter randomized clinical trial (Landi-SEP). Intensive Care Med. 2024;50:1622-1634; https://doi.org/10.1007/s00134-024-07587-1
11.Kakihana Y, Nishida O, Taniguchi T, et al. Efficacy and safety of landiolol, an ultra-short-acting β1-selective antagonist, for treatment of sepsis-related tachyarrhythmia (J-Land 3S): a multicentre, open-label, randomised controlled trial. Lancet Respir Med. 2020;8:863-872; https://doi.org/10.1016/S2213-2600(20)30037-0
12.Husereau D, Drummond M, Augustovski F, et al. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) statement: updated reporting guidance for health economic evaluations. Value Health. 2022;25(1):3-9; https://doi.org/10.1016/j.jval.2021.11.1351
13.Istituto nazionale di statistica (ISTAT). Rivaluta. Available at: https://rivaluta.istat.it/ (last accessed December 2025)
14.Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med. 2017;45:486-552; https://doi.org/10.1097/CCM.0000000000002255
15.Agenzia Italiana del Farmaco (AIFA). Lista dei farmaci in classe A. Available at: https://www.aifa.gov.it/liste-farmaci-a-h (last accessed December 2025)
16.Farmadati. Available at: https://www.farmadati.it/navigate.aspx?id=8 (last accessed December 2025)
17.Ministero della Salute. Rapporto annuale sull’attività di ricovero ospedaliero (Dati SDO 2020). 2020. Available at: https://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=3277 (last accessed December 2025)
18.Burchardi H, Schneider H. Economic aspects of severe sepsis: a review of intensive care unit costs, cost of illness and cost effectiveness of therapy. Pharmacoeconomics. 2004;22:793-813; https://doi.org/10.2165/00019053-200422120-00003
19.Accorgi D, Alti E, Barnini S, et al. Lotta alla sepsi. 2019. Available at: https://www.ars.toscana.it/lotta-alla-sepsi/toscana-agenzia-sanita-microbiologia-rischio-clinico-call-to-action-infezioni-pdta-linee-di-indirizzo.php (last accessed December 2025)
20.Agodi A, Barchitta M, Auxilia F, et al. Epidemiology of intensive care unit-acquired sepsis in Italy: results of the SPIN-UTI network. Ann Ig. 2018;30:15-21; https://doi.org/10.7416/ai.2018.2247
21.AOP Orphan Pharmaceuticals. Market research. 2024
22.Rezaei S, Matin BK, Karyani AK. Factors associated with length of stay and hospital charges among pediatric burn injury in Kermanshah, West of Iran. Journal of Pediatric Perspectives, 2015; 3(1.1): 403-409; https://doi.org/10.22038/ijp.2015.3563
23.Neifert SN, Lamb CD, Gal JS, et al. Later surgical start time is associated with longer length of stay and higher cost in cervical spine surgery. Spine (Phila Pa 1976). 2020;45:1171-1177; https://doi.org/10.1097/BRS.0000000000003516
24.Hirani R, Podder D, Stala O, et al. Strategies to reduce hospital length of stay: evidence and challenges. Medicina (Kaunas). 2025;61; https://doi.org/10.3390/MEDICINA61050922
25.Krumpl G, Walter E. Cost-effectiveness of landiolol, an ultra-short-acting beta-blocker, for treatment of sepsis related tachyarrhythmia in Germany. Pharmacoeconomics Open Access. 2023;8:1-11; https://doi.org/10.37421/2157-1042.2022.8.161
26.Arefian H, Heublein S, Scherag A, et al. Hospital-related cost of sepsis: a systematic review. J Infect. 2017;74:107-117; https://doi.org/10.1016/j.jinf.2016.11.006
27.Walter E, Heringlake M. Cost-effectiveness analysis of landiolol, an ultrashort-acting beta-blocker, for prevention of postoperative atrial fibrillation for the Germany health care system. J Cardiothorac Vasc Anesth. 2020;34:888-897; https://doi.org/10.1053/J.JVCA.2019.11.003
28.Si X, Yuan H, Shi R, et al. Comparison of the efficacy and safety of landiolol and esmolol in critically ill patients: a propensity score-matched study. Ann Intensive Care. 2025;15:1-10; https://doi.org/10.1186/S13613-024-01418-8
29.Domanovits H, Wolzt M, Stix G. Landiolol: pharmacology and its use for rate control in atrial fibrillation in an emergency setting. Eur Heart J Suppl. 2018;20:A1-A3; https://doi.org/10.1093/EURHEARTJ/SUX037